Why People Choose Fertility Preservation: Egg Freezing, Medical & Personal Reasons
Fertility preservation gives people options. It allows individuals to extend their reproductive timeline when age, medical treatment, or life circumstances make timing uncertain. At the UCSF Center for Reproductive Health, fertility preservation is both a medical intervention and a deeply personal decision shaped by each patient’s goals. Below we explain why people choose preservation, how it works, who it helps, and what to expect when you come to us.
What fertility preservation is and how it works
Fertility preservation uses cryopreservation to store eggs, sperm, or embryos for future use. The cryopreservation process typically relies on vitrification, an ultra-rapid freezing method that transforms cells into a glass-like state while preventing damage from ice crystals. When needed, these cells are thawed and used in an in vitro fertilization cycle.
Medical reasons: protecting fertility during treatment
For many patients, fertility preservation is time-sensitive. Cancer treatments such as chemotherapy and radiation can significantly impact reproductive health. That is why oncofertility care is designed to move quickly and coordinate closely with oncology teams.
Reassuringly, research from UCSF and collaborators shows that fertility preservation is both safe and effective in this setting. A 2020 study found that undergoing fertility preservation before breast cancer treatment did not negatively impact disease-free survival. In addition, a 2017 study demonstrated that random-start ovarian stimulation, a protocol used to avoid delays, does not postpone the start of chemotherapy.
Other medical reasons include:
- Conditions that affect ovarian or testicular function, for example severe endometriosis or some autoimmune diseases.
- Genetic risks that may affect fertility or risk passing on a condition. Genetic counseling is available to discuss testing and reproductive options.
- Planned medical interventions such as gonadotoxic therapies or gender-affirming treatments that may affect future fertility.
At UCSF CRH our Fertility Preservation Program offers rapid access, coordinated planning with oncology and other specialty teams, and a full suite of preservation options including egg, embryo, sperm, and ovarian tissue cryopreservation.

Endometriosis and fertility preservation
Fertility preservation is also an important consideration for patients with endometriosis, particularly those with endometriomas (ovarian cysts associated with endometriosis).
Endometriomas can impact ovarian reserve over time. In some cases, surgery to remove them is recommended to manage pain or other symptoms. However, surgery itself can further reduce ovarian reserve, which may affect future fertility.
For patients who are not ready to pursue pregnancy but want to keep their options open, fertility preservation may be recommended before surgery. Freezing eggs or embryos at this stage can help preserve reproductive potential.
At UCSF, we work closely with minimally invasive gynecologic surgeons and other specialists to identify patients who may benefit from fertility preservation and ensure timely referral and coordinated care.
Elective fertility preservation: elective and social reasons
Fertility preservation is not always driven by urgency. Many patients choose to freeze eggs or sperm as part of long-term life planning. Elective egg freezing, in particular, has grown significantly as more women seek to preserve fertility while pursuing career, education, or personal goals.
Elective sperm banking is also used by men who want future flexibility, for example before a vasectomy or when delaying fatherhood for personal or career reasons.

Social and personal factors that influence the decision include career goals, relationship timing, financial readiness, and personal comfort with assisted reproduction. Decisions are highly individual. Our team helps each person weigh medical data, success probabilities, costs, and personal values.
Research from UCSF highlights how impactful this decision can be. A 2023 study found that only 9% of women who chose to freeze their eggs reported moderate to severe regret, compared to 51% of women who considered but did not proceed. Access to clear information and support was strongly associated with greater confidence in decision-making.
Fertility preservation for transgender and gender diverse people
For transgender and gender diverse individuals, fertility preservation offers the opportunity to build a biological family before starting gender-affirming care that may impact fertility.
Options such as sperm banking, egg freezing, or embryo freezing can be completed prior to hormone therapy or surgery. Our team provides inclusive care that respects each patient’s identity while helping them navigate both medical and emotional considerations.

A closer look at egg freezing
Egg freezing is one of the most commonly used fertility preservation options today. At UCSF CRH, we guide patients through every step, from initial consultation to long-term planning.
Who is a candidate
We see patients with a range of ages and circumstances. Age matters because egg quality and quantity change over time. Egg freezing tends to be most effective when done earlier. Patients in their early 40s can still consult with us, but we will discuss the relative chances of success and alternative options.
The process
- Ovarian stimulation: Medications (FSH and LH or combinations) are given as injections for about 9 to 12 days to grow multiple follicles. Monitoring usually involves 5 to 6 clinic visits for ultrasounds and blood tests. A trigger medication times final egg maturation.
- Egg retrieval: A minimally invasive outpatient procedure performed under IV sedation. A transvaginal ultrasound guides a needle to retrieve eggs. The procedure takes about 30 minutes and same day recovery is common.
- Freezing: Mature eggs are vitrified in the lab and stored for future use.
What to expect
Egg freezing increases flexibility but is not an “insurance policy.” Outcomes depend on age at freezing, number of eggs retrieved, and future health factors. Our team provides individualized counseling to help patients understand their specific chances of success.
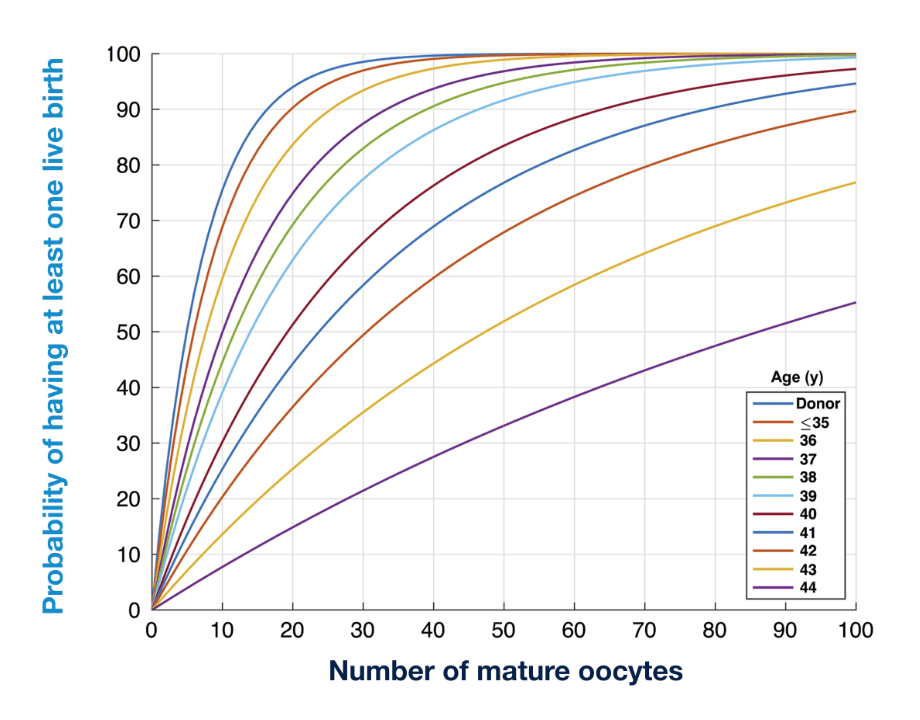
Citation: Goldman et al, Human Reproduction, 2017
BWH Egg Freezing Counseling Tool (EFCT)
Please note: These are estimates taken from outcomes of patients with infertility, NOT specifically on patients coming back to use previously frozen eggs – therefore they likely represent an overestimate of the number of eggs actually needed.
Oncofertility and outcomes after treatment
Many patients ask whether they will be able to build a family after cancer. The answer is often yes, and fertility preservation can play an important role.
Research shows encouraging outcomes. A 2021 UCSF-led study found that many patients who regained ovarian function after chemotherapy were able to conceive, either naturally or with assisted reproductive technology. These findings highlight that fertility preservation is one part of a broader continuum of care that supports family building after treatment.
For people facing cancer we prioritize speed and coordination. Our Fertility Preservation Program works with oncology teams so you can understand options quickly and receive care without unnecessary delay. Services include ovarian tissue cryopreservation, oocyte and embryo freezing, sperm cryopreservation, and specialized stimulation protocols such as random-start stimulation when timing is constrained.
We also provide follow-up reproductive health assessment after treatment, genetic counseling when relevant, and psychological support during decision making.
A decision shaped by many factors
Fertility preservation decisions are rarely based on a single factor. Instead, they reflect a combination of:
- Medical needs and timing
- Age and reproductive biology
- Career and life goals
- Financial considerations
- Personal values and support systems
At UCSF CRH, we take a multidisciplinary approach that includes physicians, embryologists, genetic counselors, and reproductive psychologists. This ensures that patients receive both the clinical expertise and emotional support needed to make informed decisions.
Moving forward
Fertility preservation is about creating options. Whether driven by a medical diagnosis, future planning, or gender-affirming care, the goal is the same: to give patients more control over when and how they build their families.
If you are considering fertility preservation, our team is here to help you understand your options and create a plan that aligns with your goals.
CITATIONS:
Letourneau, J.M., Wald, K., Sinha, N., Juarez-Hernandez, F., Harris, E., Cedars, M.I., McCulloch, C.E., Dolezal, M., Chien, A.J. and Rosen, M.P. (2020), Fertility preservation before breast cancer treatment appears unlikely to affect disease-free survival at a median follow-up of 43 months after fertility-preservation consultation. Cancer, 126: 487-495. https://doi.org/10.1002/cncr.32546
Joseph M. Letourneau, Nikita Sinha, Kaitlyn Wald, Eve Harris, Molly Quinn, Tal Imbar, Evelyn Mok-Lin, A. Jo Chien, Mitchell Rosen, Random start ovarian stimulation for fertility preservation appears unlikely to delay initiation of neoadjuvant chemotherapy for breast cancer, Human Reproduction, Volume 32, Issue 10, October 2017, Pages 2123–2129, https://doi.org/10.1093/humrep/dex276
Jaswa, E.G., Pasch, L.A., McGough, A. et al. Decision regret among women considering planned oocyte cryopreservation: a prospective cohort study. J Assist Reprod Genet 40, 1281–1290 (2023). https://doi.org/10.1007/s10815-023-02789-w
Abel, M.K., Wald, K., Sinha, N. et al. Conception after chemotherapy: post-chemotherapy method of conception and pregnancy outcomes in breast cancer patients. J Assist Reprod Genet 38, 1755–1765 (2021). https://doi.org/10.1007/s10815-021-02133-0
About Blog
There are many causes of infertility. For a successful pregnancy to occur, a healthy egg needs to meet healthy sperm, fertilize, develop and find a good place to grow (a receptive uterus). Problems at any of these steps can cause difficulties in getting pregnant. A woman’s body might not release an egg each month due to hormone imbalances, or perhaps the man’s body isn’t producing enough motile sperm.